
Exploring Determinants of Patient Adherence to Cervical Pre-Cancer Treatment in Harare, Zimbabwe
Dr. Belinda Mutibura, is an AWACAN-ED Scholar at the University of Zimbabwe, here she shares her perspective on improving cervical cancer diagnosis and describes the research she will undertake during her masters.
 Cervical pre-cancer poses a significant health burden for women worldwide, with treatment adherence playing a pivotal role in determining patient outcomes.
Cervical pre-cancer poses a significant health burden for women worldwide, with treatment adherence playing a pivotal role in determining patient outcomes.
The primary cause of cervical cancer is persistent infection with carcinogenic human papillomavirus (HPV) [1]. 10%–20% of women display a persistent infection prior to cervical carcinogenesis [2]. Additionally, women living with HIV are six times more likely to develop cervical cancer as HIV has an indirect role in oncogenesis, enhancing the effects of high-risk HPV.
Cervical cancer is one of the most preventable and treatable forms of cancer, provided it is detected early and managed effectively [3]. This is primarily achieved through regular screening to identify and promptly treat precancerous lesions. Screening methods such as Visual Inspection with Acetic acid and Camera (VIAC), cervical cytology smear, and HPV DNA testing are vital tools in early detection [3].
Treatment methods for pre-cancerous lesions may be ablative or excisional. According to a Cochrane review, cure rates for high-grade precancerous lesions (CIN III) following cryotherapy an ablative treatment range from 77%-93% [4]. In another Cochrane review for excisional techniques using the Loop electrosurgical excision procedure, a cure rate of 91-98% has been reported. [4].
In 2012 Zimbabwe rolled out a National Cervical Cancer screening program by adopting the VIAC in public health facilities, with a screen and treat approach. Women between the ages of 25- 49 years are eligible for screening and current coverage is 20% of eligible women [5] [6]. In Harare between 2014 and 2016, there was a 35% drop in the number of women utilizing VIAC services, with a VIAC positive screen prevalence range of 5.8 to 7.4% [6]. Furthermore, 74.1% of the women who screened positive did not receive treatment at the same site where the screening took place [6]. Therefore, not recognizing the screen and treat approach.
Cervical cancer screening as a standalone pillar has no actual preventive value. The success of screening programs is heavily reliant on the adherence of patients to the recommended treatment protocols following a positive screening result.
Despite the availability of effective screening and treatment modalities for cervical pre-cancer, Zimbabwe faces challenges with patient adherence to these strategies. Low adherence rates significantly increase the risk of disease progression. Understanding the factors that influence patient adherence to cervical precancer treatment is crucial in improving outcomes and reducing the burden of cervical cancer.
Research objectives
The aim of this study is to identify factors influencing adherence to cervical cancer pre-cancer regimens in Harare, Zimbabwe by addressing the following:
Quantitative research objectives
- Quantifying rates of adherence to treatment among women with test positive VIAC screening test result
- Analyzing the variation in adherence rates between women living with HIV and HIV-negative women.
- Documenting the time interval from screening to treatment among women with VIAC test positive results.
Qualitative research objectives
- Exploring socio-demographic, behavioral, and health system factors affecting adherence to treatment.
- Exploring how the Health Belief Model influences adherence to treatment of cervical cancer precancerous conditions.
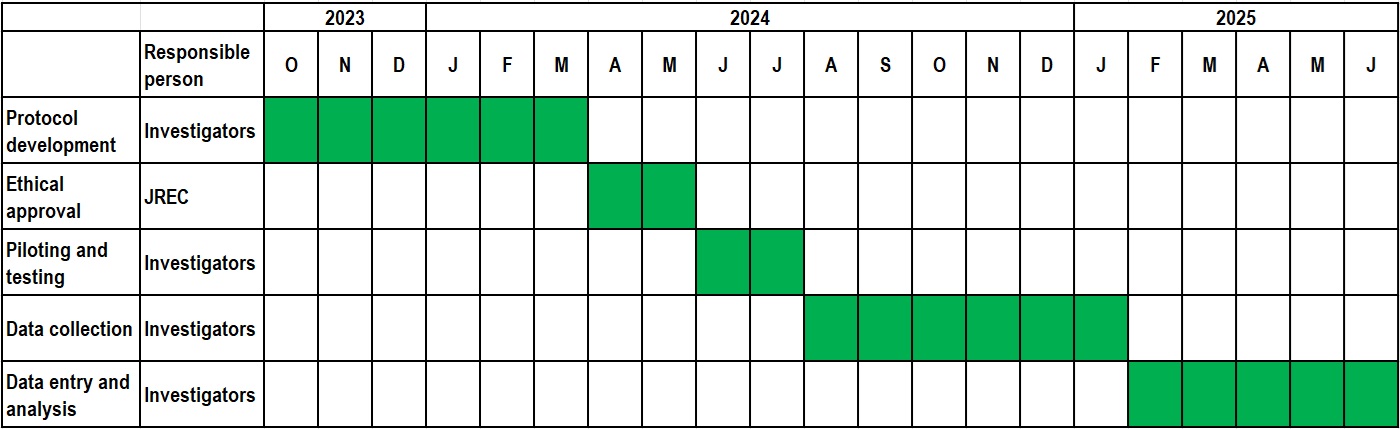
Research outline
Outcomes and impact
- Enhanced Understanding of Adherence Dynamics
- Development of Targeted Interventions
- Policy and Healthcare Practice Recommendations
- Contribution to Global CC Elimination Efforts
- Potential to Inform Future Research
In summary, the expected outcomes and implications of this study are far-reaching, with the potential to significantly impact both the theoretical understanding of treatment adherence and practical aspects of cervical cancer prevention and management. The integration of these findings into public health strategies and clinical practice could have a meaningful impact on reducing the incidence and mortality associated with cervical cancer in Zimbabwe and similar contexts.
References
- J. M.Walboomers et al, “Human Papillomavirus is a necessary cause of invasive cervical cancer worldwide,” J Pathol, vol. 12, p. 189, 1999
- P.E. Gravitt, “The known unknowns of HPV natural history,” J Clin Invest, pp. 4593-4599, 2011
- World Health Organization, Global strategy to accelerate the elimination of cervical cancer as a public health problem, Nov 2020, www.who.int/publications/i/item/9789240014107
- M. Maza et al, “Cervical Precancer treatment in low- and middle income countries: A technology overview,” J Glob Oncol, pp. 400-408, 2016
- Ministry of Health and Child Care, Zimbabwe, The National Cancer Prevention and Control Strategy For Zimbabwe 2014–2018, 2017
- C.Gabaza et al, “Utilization and outcomes of cervical cancer screening services in Harare City, 2012-2016: a secondary data analysis,” BMC health service research, p. 454, 2019
 Belinda is a postgraduate student in obstetrics and gynaecology with an interest in gynaecological cancers. She has been working in the department of obstetrics and gynaecology for 4 years.
Belinda is a postgraduate student in obstetrics and gynaecology with an interest in gynaecological cancers. She has been working in the department of obstetrics and gynaecology for 4 years.